1601006186 (long case)
Demographics
34 year old male, labourer by occupation, from Narketpalli
Chief complaints
Fever since 10 days
Cough since 7 days
Breathlessness since 4 days
Presenting illness
Patient was apparently asymptotic 1 month back, then developed
Breathlessness which is invidious onset grade III(MMRC) and progressed from grade III to grade IV, not associated with postural variation or diurnal variation. Generalised weaknesses followed by low grade fever associated with chills, rigor, shows no diurnal variation, and
cough since 7 days, associated with moderate amount of purulent sputum mixed with saliva , no postural variation, no loss of smell

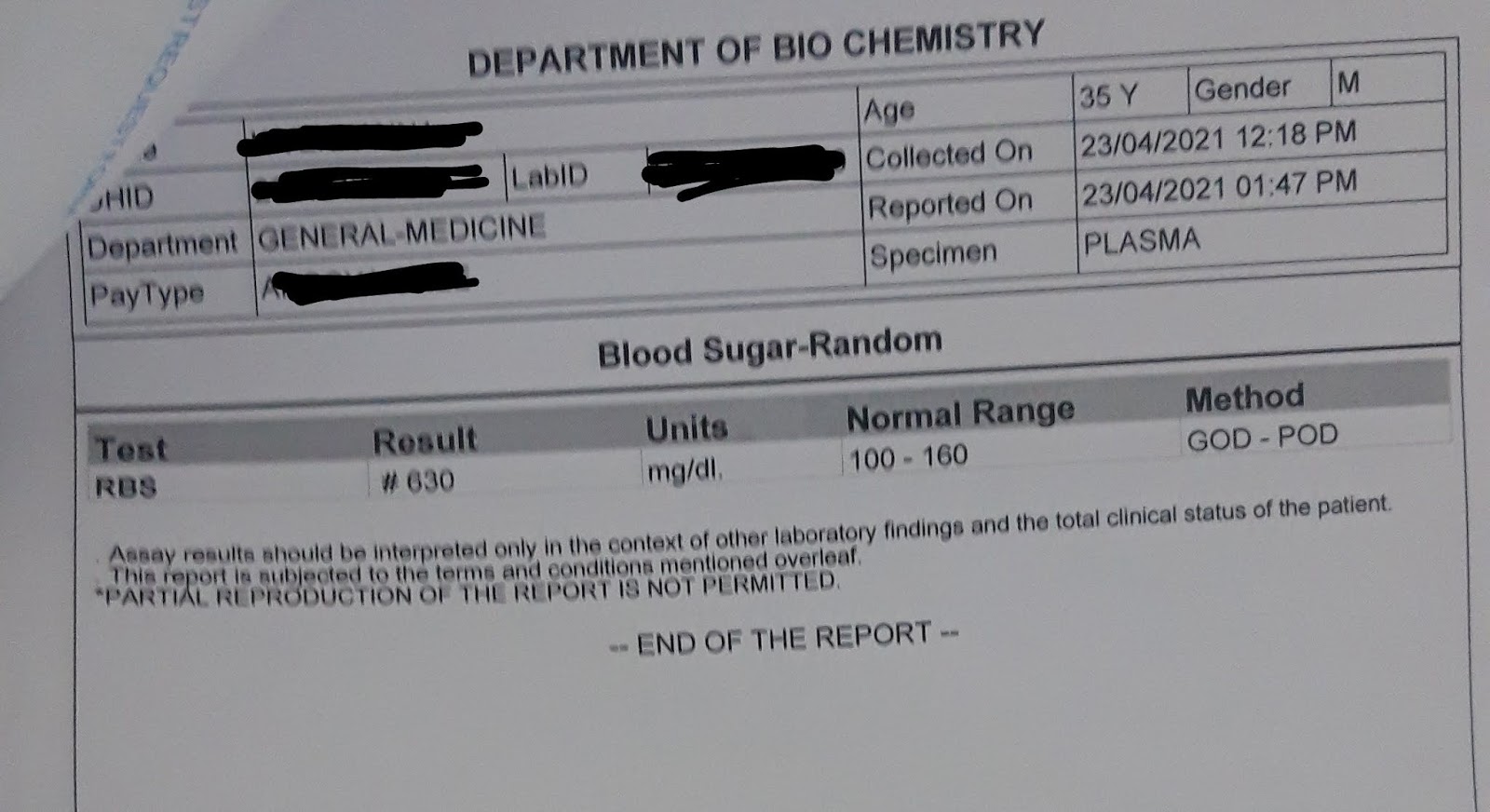
Complaints of polyuria, polydipsIa, polyphagia since 2 months
No complaints of Palpitation, syncopal attack, cheats pain, haemoptysis, recurrent sore throat, hoarseness, choking episode, burning miturirition, loose stools, constipation.
Past history
Not a known case of DM, hypertension, epilepsy, asthma, CVD, TB, thyroid disease
Family history
None of patients attenders have similar symptoms, or have asthma, TB, hypertension, DM, CVD.
Personal history
Diet mixed
Appetite decreased
Sleep adequate
Alcohol consumption 70ml/day
Bladder and bowel regular
Drug history
No known drug allergies
Was on IV RL
General examination
After taking concent
I examined patient in supine and sitting position.
Patient is conscious coherent cooperative well oriented to time place person, has wasting of muscles, is comfortable on bed.
There is no pallor, icterus, cyanosis koilonychias, clubbing, lymphadenopathy, pedal edema
JVP is not elevated, hepatojuglular reflex absent.
Vitals
Pulse rate 100 beats/min regular in rhythm character volume
Blood pressure 90/70 mmHg left arm in sitting position.
Respiratory rate 40 cycles per minute
Spo2 98% on room air.

Respiratory Systemic examination
1. Upper airway
Nose normal alae Nasi, septum
Oral cavity teeth pharynx normal no sinus tenderness
2. examination of chest
INSPECTION
Shape of chest elliptical
Trachea central
Apical impulse 5 inter coastal space medial to mid-clavicular line
Skin over chest is normal
Trail sign is absent
Supra clavicular and supra scapular hollwing is present



PALPATION
No local rise of temperature
No tenderness
Chest is expanding equally on both sides
Tactile vocal fremitus is increased infra axillary infra scapular areas both sides
No palpable thrills capitation pleural rub
PERCUSSION
Direct percussion on clavicle sternum and Manubrium is resonant
Kronig isthmus resonant both sides
Indirect percussion(left) anteriorly mid claviclular line 2-6 intercostal spaces are resonant. Laterally mid axillary line 4 intercostal spaces are resonant, 5-7 intercostal spaces dull, posterity 9th intercostal space dull
Indirect percussion(right) anteriorly mid claviclular line 2-6 intercostal spaces are resonant. Laterally mid axillary line 4-5 intercostal spaces are resonant, 6,7 intercostal space are dull. posterity 9th intercostal space dullTraube space dull
AUSCULTATION
Left side supraclavicular, infraclavicular, mammary, inframammary, suprascapular, normal vesicular breath sounds, decreased (bronchial) breath sounds at infraaxillary, scapular, infrascapular areas. Crepetations at infra scapular area
Right side supraclavicular, infraclavicular, mammary, inframammary, suprascapular, normal vesicular breath sounds, decreased breath sounds at infraaxillary, infrascapular areas.
Vocal resonance increased at infraaxillary, infrascapular areas on left side.
Other system examination
CNS - higher mental functions normal, cranial nerves normal, motor system normal, Reflexes normal, sensory system normal, no meningeal signs, no cerebellar signs
CVS - no visible pulsations, apical impulse on 5th intercostal space 1cm medial to mid clavicular line. S1 S2 heard no added murmurs
ABDOMEN - abdomen is scaphoid with all quadrants moving equally with respiration, umbilicus central and inverted, no abdominal tenderness, no organomegaly
Complete blood picture

Serum electrolytes

Arterial blood gas

Urine for ketone bodies

Blood urea


Serum creatinine

Chest X-Ray
21 Apr 2021



Provisional Diagnosis
Case of left lower lobe community acquired pneumonia. With possible diabetic ketosis.


Comments
Post a Comment